Originally published by our sister publication General Surgery News

Ahsun Riaz, MD
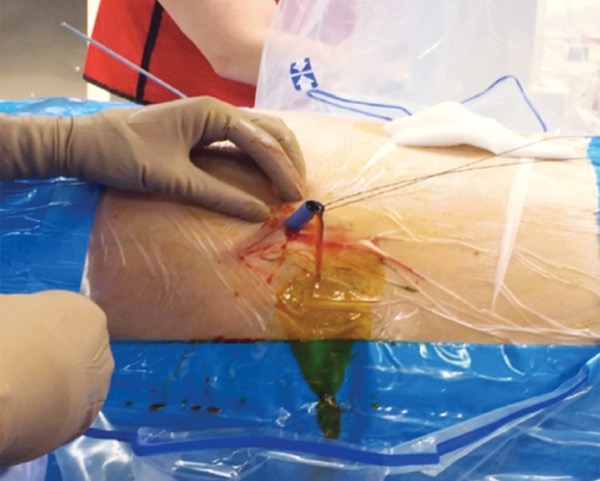
CLEVELAND—Surgery is not the only therapeutic option available to treat gallstones, according to an expert in the field. As Ahsun Riaz, MD, discussed, percutaneous approaches can be used in a specific subset of patients in whom surgery is neither safe nor viable.
“The thing we’ve recognized at Northwestern is that percutaneous cholecystostomies are not definitive