Originally published by our sister publication Pharmacy Practice News

Bonnie Kirschenbaum, MS, FASHP, FCSHP
“Reimbursement Matters” is a tool for maintaining your health system’s fiscal health. Please email the author at bonniekirschenbaum@gmail.com with suggestions on reimbursement issues that you would like to see covered.
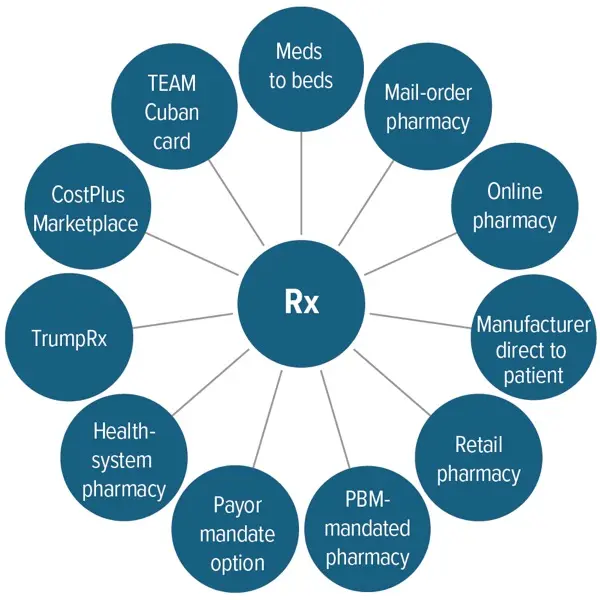
Each new year brings change to how healthcare is offered and paid for. Some of those changes are opportunities for pharmacy to provide more services to