Originally published by our sister publication Anesthesiology News

Maximilian S. Schaefer, MD
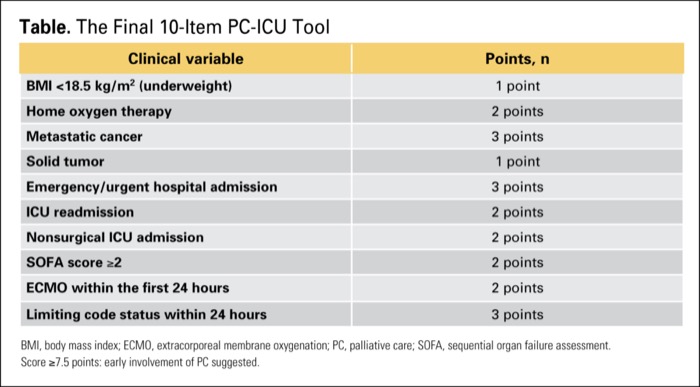
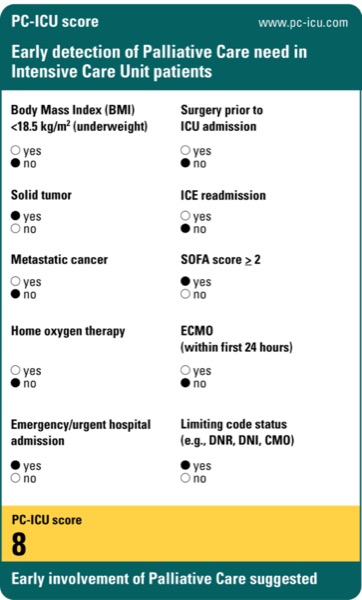
The development of a novel scoring system may make it easier to identify ICU patients who need palliative care (PC). According to a recent study, the PC-ICU score has good discriminative ability, and an abbreviated version of the score—which clinicians may find easier to use—demonstrated comparable performance.
“Palliative care is not just about end-of-life care, but can also improve