Originally published by our sister publication Anesthesiology News

Department of Rehabilitation and Human Performance
Icahn School of Medicine at Mount Sinai
New York City
Icahn School of Medicine at Mount Sinai
New York City
Department of Anesthesiology, Critical Care and Pain Management
Hospital for Special Surgery
Department of Anesthesiology
Weill Cornell Medicine
New York City
Hospital for Special Surgery
Department of Anesthesiology
Weill Cornell Medicine
New York City
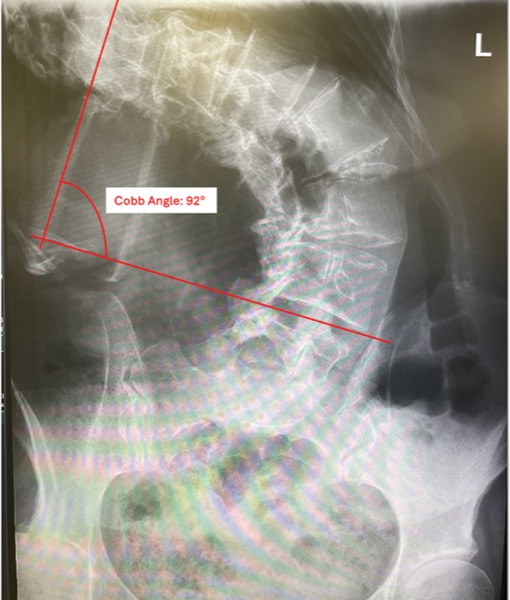
For patients with severe scoliosis, careful preoperative planning is paramount for intraoperative and postoperative care