Originally published by our sister publication Anesthesiology News
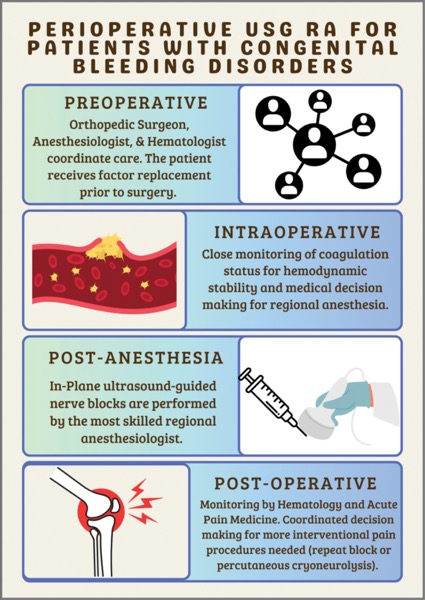
SAN DIEGO—Peripheral nerve blocks appear to be safe in patients with congenital bleeding disorders in the immediate postoperative period, according to a study presented at the 2024 annual spring meeting of the American Society of Regional Anesthesia and Pain Medicine (abstract 5502).
However, researchers at The University of Texas Health Science Center at Houston noted that coagulation factors must first be optimized by a