Originally published by our sister publication Pharmacy Practice News
The title “When the Good Times Roll Too Far: An Overview of ‘Party Drug’ Management” proved to be apt for a session at the ASHP Midyear 2024 Clinical Meeting & Exhibition, in New Orleans. It attracted so much interest that not one, but two, overflow rooms were needed to accommodate the crowd.
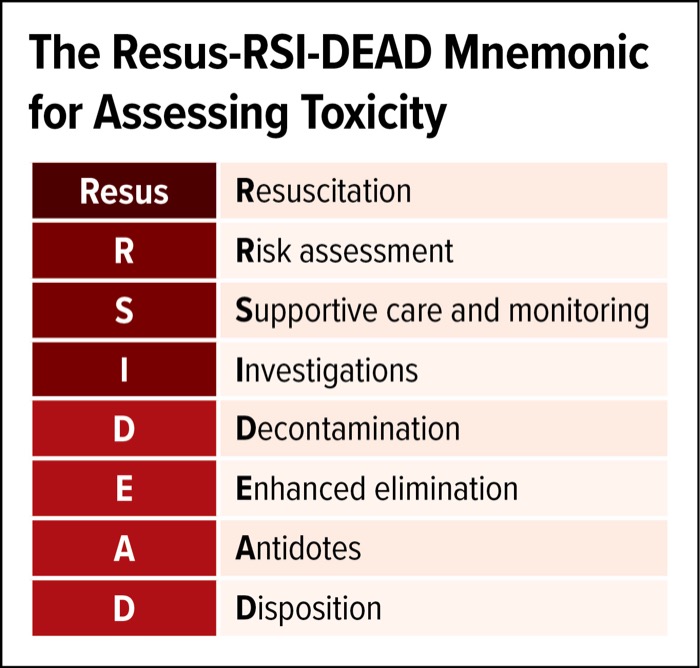
What caused the excitement? Three emergency department (ED) clinical